{kind=link}

Patellofemoral ache syndrome (PFPS) is a time period that describes generalized anterior knee ache round or underneath the patella. Overactivity and extreme mechanical load on the patellofemoral joint are the main causes. There isn’t an obvious tissue dysfunction for the ache, however a number of elements could contribute to the discomfort felt throughout motion.
Under we focus on key anatomical, biomechanical, and psychosocial elements that play a job on this difficult drawback. Therapeutic massage remedy remedy for PFPS is most profitable when the practitioner understands the basics of the joint mechanics, elements within the consumer’s actions, and way of life, and might mix these parts with particular evaluation findings to assemble a helpful remedy technique.
Anatomical Background
PFPS is difficult as a result of it isn’t clear what’s inflicting the ache generally.1 Nonetheless, an excellent understanding of knee anatomy and mechanics helps determine key contributors to the issue. The primary place to start out is with the knee extensor muscle group.
The big and highly effective quadriceps femoris muscle group is answerable for knee extension. Whereas extension happens on the tibiofemoral joint (between the femur and tibia), a 3rd bone, the patella, is an integral a part of energy technology for this motion. The patella has a bony ridge on its underside (Picture 1). That ridge suits within the groove between the 2 femoral condyles. The patella strikes superiorly and inferiorly throughout flexion and extension, and the bony ridge tracks in a groove shaped by the femoral condyles.
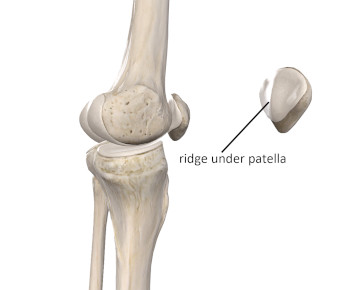
Picture 1
Picture courtesy of Full Anatomy
The patella is a sesamoid (floating) bone embedded within the quadriceps (patellar) tendon. Apparently, infants are born with out a patella. The bone develops within the tendon because the child progressively begins rising load by weight-bearing and standing. Anatomy books primarily present the 4 quadriceps muscle groups mixing into the patellar tendon and attaching to the tibial tuberosity. Nonetheless, drive can also be transmitted to the tibia by the use of connective tissues across the knee that make up the quadriceps retinaculum (Picture 2). The quadriceps retinaculum is richly innervated, so it’s more likely to be a supply of ache with mechanical challenges of PFPS.2
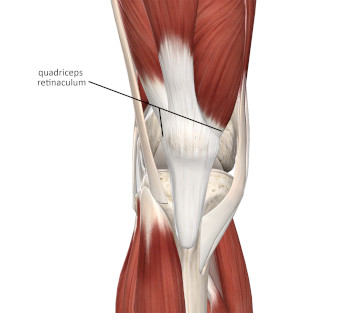
Picture 2
Picture courtesy of Full Anatomy
Whereas the patella does supply some safety for the knee, its main function is enhancing mechanical operate on the joint. Drive manufacturing at a joint relies on a physics precept known as the second arm. So, what on earth is a second arm (it has nothing to do with time or the higher extremity)? Most joint actions happen round some extent known as the axis of rotation. Envision an imaginary rod going by the knee joint proper on the axis of rotation, with the tibia rotating round that rod throughout flexion and extension. The second arm is the size between the joint’s axis of rotation and the road of drive that acts on the joint (Picture 3). The first operate of the patella is to extend the size of the second arm for knee extension, which makes the quadriceps extra highly effective. These increased drive masses throughout knee extension and flexion may also be a contributing issue to patellofemoral ache.
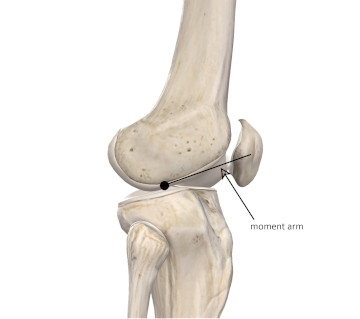
Picture 3
Picture courtesy of Full Anatomy
What Causes Patellofemoral Ache?
PFPS is most typical in younger folks, particularly these between the ages of 12 and 17 concerned in operating, leaping, or different vigorous decrease extremity exercise. But, the situation can also be prevalent in folks all through all age ranges who abruptly enhance exercise masses or do one thing that includes excessive drive masses throughout knee flexion and extension. Overactivity seems to be the most important drawback.
Girls develop PFPS extra usually than males, though the explanations for this should not absolutely clear. A number of elements play a job in that elevated incidence. The primary is a bigger Q angle in ladies. The Q angle, additionally known as the quadriceps angle, is shaped by imaginary strains that join bony landmarks. One line extends from the tibial tuberosity by the midpoint of the patella. One other line passes from the ASIS to the midpoint of the patella. The angle between these strains is the Q angle (Picture 4). The broader is the pelvis, as happens in females, the bigger is the Q angle. The quadriceps pull extra laterally when the Q angle is bigger and never as a lot straight up and down. The elevated lateral pull from the quadriceps pulls the patella in a extra lateral course, leading to patellar monitoring issues that change into a main issue within the consumer’s PFPS ache.
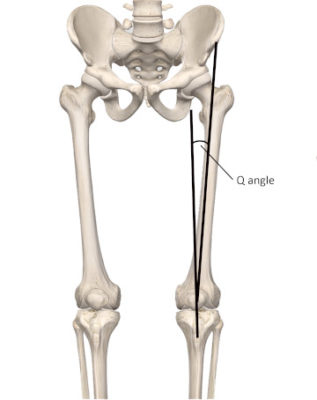
Picture 4
Picture courtesy of Full Anatomy
There may be additionally an elevated incidence of valgus (knock-knee tendency) alignment on the knee in ladies. The elevated valgus alignment additionally causes the quadriceps to tug extra in a lateral course. Different postural alignments within the decrease extremity can even play a job. Elevated foot pronation throughout gait could also be one other potential explanation for alignment and corresponding patellar monitoring issues.
Weak point within the hip abductors or exterior rotators may contribute to the issue. When the exterior hip rotators are weak, the femur could also be pulled towards medial rotation. With the hip extra medially rotated throughout knee flexion and extension, the patella tends towards lateral monitoring. As we will see, most of those alignment issues contain the patella monitoring an excessive amount of laterally and never straight up and down.
Probably the most distal portion of the vastus medialis within the quadriceps muscle group capabilities to offset the lateral pull on the patella. Due to the indirect orientation of those vastus medialis fibers, this portion of the muscle known as the vastus medialis obliquus or VMO.
PFPS is carefully associated to a different situation known as chondromalacia patella. Chondromalacia is softening and degeneration of the articular cartilage. When the patella is repeatedly pulled in opposition to the femoral condyles, as in a monitoring dysfunction, it might trigger degradation and breakdown of the articular cartilage on the underside of the patella. Cartilage degeneration is obvious with grinding or grating sensations of the patella throughout knee flexion and extension.
Previously, the ache of patellofemoral ache syndrome was blamed on cartilage degeneration. But, the hyaline cartilage underneath the patella is poorly innervated, so it’s unlikely that important knee ache comes from the cartilage degeneration itself in PFPS. Nonetheless, just below the cartilage is a layer of richly innervated subchondral bone. Ache might definitely consequence from friction of the subchondral bone.
The biomechanical elements talked about above are thought-about the commonest causes of PFPS. Nonetheless, psychosocial elements may contribute to the ache. Anxiousness, melancholy, catastrophizing (considering issues are a lot worse than they’re), and kinesiophobia (concern of motion) may contribute to the anterior knee ache of PFPS. It’s not frequent for these psychosocial elements to supply ache on their very own, however any mixture of biomechanical and psychosocial elements ought to be thought-about in an entire analysis.
Evaluation
The analysis of PFPS begins with an intensive consumer historical past. The commonest grievance is ache felt with leaping, operating, or climbing and descending stairs. Ache can also be probably when the knee stays flexed for lengthy durations, resembling an extended automobile trip or sitting in a movie show. As famous earlier, the consumer may complain of grinding or grating sensations of the patella throughout knee flexion or extension actions. You’ll be able to place your hand flippantly on the patella because the consumer is seated on the sting of the desk and transfer the knee by flexion and extension. Not a lot stress on the patella is required to really feel these grinding sensations.
The tissues surrounding the patella, particularly the quadriceps retinaculum, could also be tender when palpated. You’ll be able to palpate them with the knee in full passive extension on the remedy desk and when the knee is shifting by flexion and extension. Better tensile masses are on the retinacular tissues throughout movement, and this will increase sensitivity throughout palpation.
It could even be useful to understand the patella between your fingers and transfer it backward and forward (Picture 5). Ideally, the patella ought to transfer about half its width to every aspect. It’s not essentially pathological if it doesn’t transfer a lot, however word if considerably restricted. Particularly, word if it strikes simply in a lateral course however doesn’t transfer a lot in a medial course. This might point out tightness within the lateral restraining tissues. Additionally, connective tissue fibers from the iliotibial band lengthen into the lateral retinaculum across the quadriceps. So, tightness transmitted by the iliotibial band from the hip abductor and gluteus maximus muscle groups might additionally play a job in improper patellar monitoring.

Picture 5
Lateral motion of patella
There are a number of particular orthopedic exams generally used to judge PFPS. Nonetheless, in recent times their accuracy has been known as into query.3 It seems that a complete historical past along side some primary bodily examination procedures are nonetheless probably the most correct technique of figuring out the issue.4 Probably the most useful bodily examination elements embrace:
- Ache across the patella with palpation
- Elevated ache throughout palpation with the extensor muscle groups underneath load (resembling palpation throughout a partial squat)
- Ache with squatting or going up or downstairs
Remember that different issues across the knee could have comparable indicators and signs. These situations embrace patellar tendinosis, joint pathology, plica syndromes, Osgood-Schlatter’s illness, or ache from peripheral nerve or nerve root compression.
Therapy
The commonest therapies for PFPS are conservative and noninvasive. In conventional orthopedic therapies, patellar taping and bracing are frequent. They appear to be more practical within the quick time period versus with extra power instances. Bettering energy stability inside the quadriceps can also be a core element of bodily remedy remedy.
Therapeutic massage can clearly play a job in treating patellar monitoring problems, particularly in decreasing hypertonicity of the tissues across the patella. Decreasing hypertonicity helps restore muscular stability. The soothing results of gliding therapeutic massage strokes on a painful knee shouldn’t be undervalued both. Efficient approaches could mix strategies with a broad context floor resembling the total palm or hand, together with extra particular stripping strategies utilizing the thumb, finger, or maybe a stress software. I’ve additionally discovered performing these strategies throughout energetic motion of the knee enhances their effectiveness. You’ll be able to see an energetic engagement approach for the patellar retinaculum in this video.
Conclusion
Anterior knee ache is a typical grievance for quite a few purchasers. It’s more likely to happen with any people engaged in excessive exercise ranges. Understanding the biomechanical function of the patella and surrounding tissues may also help you goal your remedy for the most effective outcomes. Growing a greater understanding of patellofemoral operate additionally illustrates a superb alternative so that you can work with different well being professionals to attain the most effective outcomes for the consumer.
Assets consulted:
- Hott A, Brox JI, Pripp AH, Juel NG, Liavaag S. Predictors of Ache, Operate, and Change in Patellofemoral Ache. Am J Sports activities Med. 2020;48(2):351-358. doi:10.1177/0363546519889623
- Rothermich MA, Glaviano NR, Li J, Hart JM. Patellofemoral ache. Epidemiology, pathophysiology, and remedy choices. Clin Sports activities Med. 2015;34(2):313-327. doi:10.1016/j.csm.2014.12.011
- Nunes GS, Stapait EL, Kirsten MH, de Noronha M, Santos GM. Medical check for analysis of patellofemoral ache syndrome: Systematic evaluate with meta-analysis. Phys Ther Sport. 2013;14(1):54-59. doi:10.1016/j.ptsp.2012.11.003
- Willy RW, Hoglund LT, Barton CJ, et al. Patellofemoral ache medical follow pointers linked to the worldwide classification of functioning, incapacity and well being from the academy of orthopaedic bodily remedy of the American bodily remedy affiliation. J Orthop Sports activities Phys Ther. 2019;49(9):CPG1-CPG95. doi:10.2519/jospt.2019.0302
To discover different articles, take a look at our weblog: Weblog
Hearken to The Considering Practitioner podcast: Podcast